Bladder exstrophy
Overview
Bladder exstrophy (EK-stroh-fee) is a rare birth defect in which the bladder develops outside the fetus. The exposed bladder can't store urine or function normally, resulting in urine leakage (incontinence).
Problems caused by bladder exstrophy vary in severity. They can include defects in the bladder, genitals and pelvic bones, as well as defects in the intestines and reproductive organs.
Bladder exstrophy may be spotted on a routine ultrasound during pregnancy. Sometimes, though, the defect isn't visible until the baby is born. Babies born with bladder exstrophy will need surgery to correct the defects.
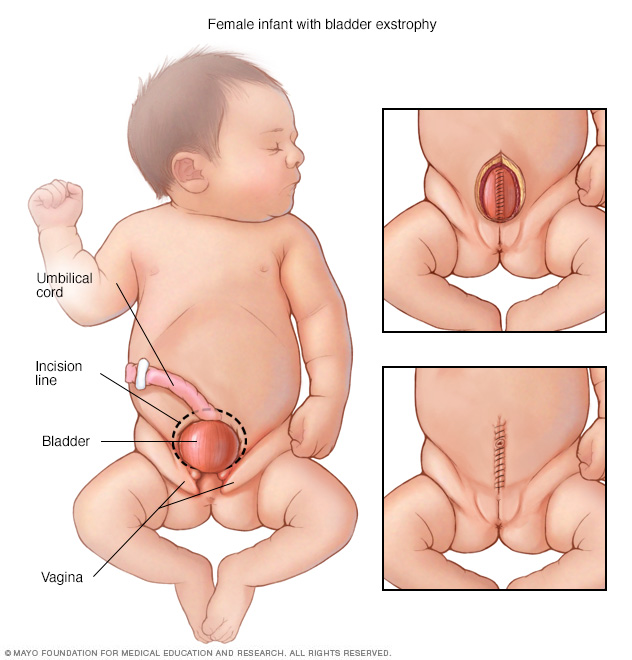
In girls born with bladder exstrophy, the bladder is on the outside of the body and the vagina is not fully formed. Surgeons will close the bladder (top right) and then close the abdomen and skin (bottom right).
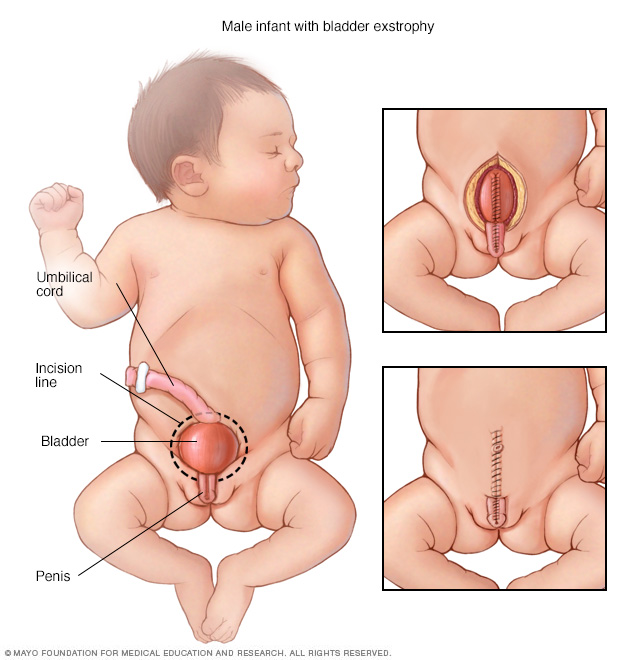
In boys born with bladder exstrophy, the bladder is on the outside of the body and the penis and the urine tube (urethra) are not fully closed. Surgeons will close the penis and bladder (top right) and then close the abdomen and skin (bottom right).
Symptoms
Bladder exstrophy is the most common in the larger group of birth defects called the bladder exstrophy-epispadias complex (BEEC). Children with BEEC have one of the following:
- Epispadias. This is the least severe form of BEEC, in which the tube to expel urine (urethra) doesn't fully develop.
-
Bladder exstrophy. This defect causes the bladder to form on the outside of the body. The bladder is also turned inside out. Usually, bladder exstrophy will involve organs of the urinary tract, as well as the digestive and reproductive systems. Defects of the abdominal wall, bladder, genitals, pelvic bones, final section of the large intestine (rectum) and opening at the end of the rectum (anus) can occur.
Children with bladder exstrophy also have vesicoureteral reflux. This condition causes urine to flow the wrong way — from the bladder back up into the tubes that connect to the kidneys (ureters). Children with bladder exstrophy also have epispadias.
-
Cloacal exstrophy. Cloacal exstrophy (kloe-A-kul EK-stroh-fee) is the most serious form of BEEC. In this condition, the rectum, bladder and genitals don't fully separate as the fetus develops. These organs may not be correctly formed, and the pelvic bones are affected as well.
The kidneys, backbone and spinal cord also may be affected. Most children with cloacal exstrophy have spinal abnormalities, including spina bifida. Children born with protruding abdominal organs probably also have cloacal exstrophy or bladder exstrophy.
Causes
The cause of bladder exstrophy is unknown. Researchers think that a combination of genetic and environmental factors likely plays a role.
What is known is that as the fetus grows, a structure called the cloaca (klo-A-kuh) — where reproductive, urinary and digestive openings all come together — doesn't develop properly in babies who develop bladder exstrophy. Defects in the cloaca can vary a lot depending on the age of the fetus when the developmental error occurs.
Risk factors
Factors that increase the risk of bladder exstrophy include:
- Family history. Firstborn children, children of a parent with bladder exstrophy or siblings of a child with bladder exstrophy have an increased chance of being born with the condition.
- Race. Bladder exstrophy is more common in whites than in other races.
- Sex. More boys than girls are born with bladder exstrophy.
- Use of assisted reproduction. Children born through assisted reproductive technology, such as IVF, have a higher risk of bladder exstrophy.
Complications
Without surgery
Without treatment, children with bladder exstrophy won't be able to hold urine (urinary incontinence). They're also at risk of sexual dysfunction and have an increased risk of bladder cancer.
After surgery
Surgery can reduce complications. The success of surgery depends on how severe the defect is. Many children who have surgical repair are able to hold urine. Young children with bladder exstrophy may walk with their legs turned somewhat outward due to the separation of their pelvic bones.
Long-term complications
People born with bladder exstrophy can go on to have normal sexual function, including the ability to have children. However, pregnancy will be high risk for both mother and baby, and a planned cesarean birth may be needed.
Diagnosis
Bladder exstrophy is found incidentally during a routine pregnancy ultrasound. It can be more definitively diagnosed before birth with ultrasound or MRI. Signs of bladder exstrophy seen during imaging tests include:
- Bladder that doesn't fill or empty correctly
- Umbilical cord that is placed low on the abdomen
- Pubic bones — part of the hipbones that form the pelvis — that are separated
- Smaller than normal genitals
Sometimes the condition can't be seen until after the baby is born. In a newborn, doctors look for:
- Size of the portion of the bladder that is open and exposed to air
- Position of the testicles
- Intestine bulging through the abdominal wall (inguinal hernia)
- Anatomy of the area around the navel
- Position of opening at the end of the rectum (anus)
- How much the pubic bones are separated, and how easily the pelvis moves
Treatment
After delivery, the bladder is covered with a clear plastic dressing to protect it.
Children born with bladder exstrophy are treated with reconstructive surgery after birth. The overall goals of reconstruction are to:
- Provide enough space for urine storage
- Create outer sex organs (external genitalia) that look and function acceptably
- Establish bladder control (continence)
- Preserve kidney function
There are two main approaches to surgery, though it's not clear whether one approach is significantly better than the other. Research is ongoing to refine the surgeries and study their long-term outcomes. The two types of surgical repair include:
- Complete repair. This procedure is called complete primary repair of bladder exstrophy. Complete repair surgery is performed in a single procedure that closes the bladder and the abdomen and repairs the urethra and outer sex organs. This can be done soon after birth, or when the baby is around two to three months old.
Most surgery for newborns will include repair to the pelvic bones. However, doctors may choose not to do this repair if the baby is less than 72 hours old, the pelvic separation is small and the infant's bones are flexible.
Staged repair. The full name of this approach is modern staged repair of bladder exstrophy. Staged repair involves three operations. One is done within 72 hours after birth, another at age 6 to 12 months, and the last at 4 to 5 years.
The first procedure closes the bladder and the abdomen, and the second repairs the urethra and sex organs. Then, when the child is old enough to participate in toilet training, surgeons perform bladder neck reconstruction.
Surgical follow-up
Standard care after surgery includes:
- Immobilization. After surgery, infants need to stay in traction while they heal. The amount of time a child needs to be immobilized varies, but is typically around four to six weeks.
- Pain management. Doctors can place a thin tube into the spinal canal during surgery to deliver pain medications directly to the area it's needed. This allows for more consistent pain control and less use of opioid medications.
After surgery, most — but not all — children will be able to achieve continence. Children sometimes need to have a tube inserted into their bladders to drain urine (catheterization). Additional surgeries may be needed as your child grows.
Coping and support
Having a baby with a significant and rare birth defect such as bladder exstrophy can be extremely stressful. It's difficult for doctors to predict how successful surgery will be, so you're facing an unknown future for your child.
Depending on the surgery's outcome and the degree of continence after surgery, your child may experience emotional and social challenges. A social worker or other behavioral health professional can offer your child and your family support in facing these challenges.
Some doctors recommend that all children with BEEC receive early counseling and that they and their families continue to receive psychological support into adulthood.
You may also benefit from finding a support group of other parents who are dealing with the condition. Talking with others who've had similar experiences and understand what you're going through can be helpful.
It may also be helpful to keep in mind that children with bladder exstrophy have normal life expectancies, and a good chance of living full, productive lives with work, relationships and children of their own.
Preparing for an appointment
Your health care provider may have diagnosed your baby's condition during your pregnancy. If so, in addition to the health care provider you've selected to care for you during your pregnancy, you'll also likely consult with a multidisciplinary team of physicians, surgeons and other specialists.
Here's some information to help you get ready for your appointment, and what to expect from your health care providers if your unborn baby has been diagnosed with bladder exstrophy.
What you can do
- Be aware of any pre-appointment instructions. At the time you make the appointment, be sure to ask if there's any special preparation needed.
- Ask a family member or friend to come with you, if possible. Sometimes it can be difficult to remember all the information provided to you during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Write down questions to ask your doctor. Preparing questions ahead of time will help you make the most of your time with your health care providers.
For bladder exstrophy, some basic questions to ask include:
- What is the extent of the defect? Can you tell how severe it is?
- Can my baby be treated during pregnancy?
- What will be done for my baby immediately after birth?
- Will the treatment cure my child?
- How many and what types of surgeries will my child need?
- What are some of the potential complications of treatment or surgery?
- Will there be any lasting effects?
- Are there any support groups that can help my child and me?
- What are the odds of this happening again in future pregnancies?
- Is there any way to keep this from happening again in the future?
- What websites do you recommend visiting?
In addition to the questions that you've prepared to ask your doctor, don't hesitate to ask other questions during your appointment.
What to expect from your doctor
Your doctor is likely to ask you a number of questions, such as:
- Have you ever had a child with bladder exstrophy or other birth defects?
- Has anyone in your family been born with bladder exstrophy?
- If necessary, are you able to travel to a facility that offers specialized care?
Last Updated Feb 11, 2022
© 2024 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use


